


Deep Dive: Lipid Nanoparticle siRNA Drugs Patisiran and Inclisiran
I think Peter McCullough is forecasting another bright future... 🤨

I regret to say that this post will not be a short journey today. I will do my best to lay out what I see as concisely as possible. But just like any other aspect of this op, there are just so many layers to peel away.
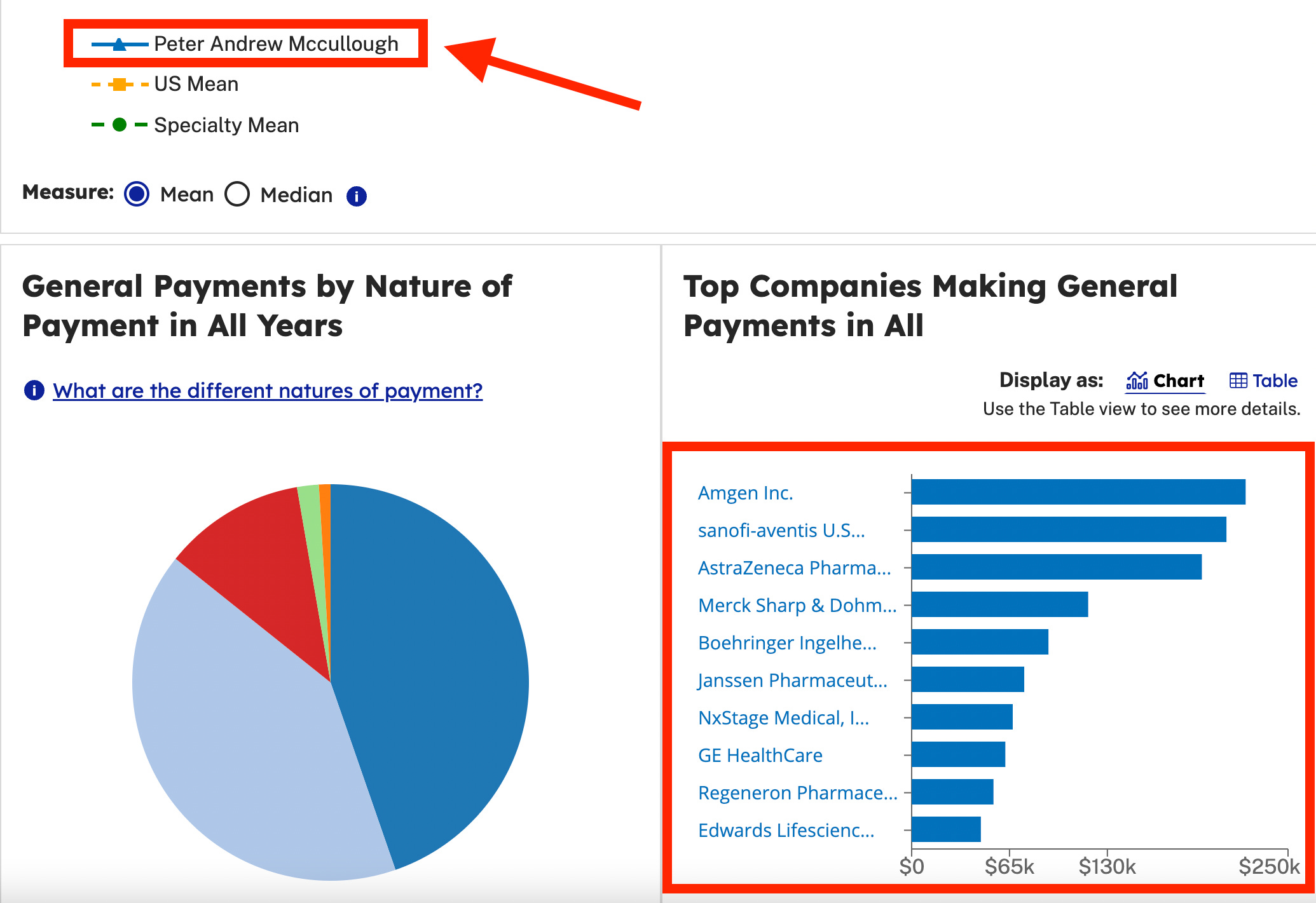
The rabbit hole down which I currently find myself began a week or so ago, with Peter McCullough’s rather shocking endorsement of siRNA to combat the mRNA injections that have been deployed around the world.
I found it stunning that a doctor so outspoken about the harms of mRNA, would nonchalantly suggest injecting some siRNA to negate the previously injected mRNA.
Considering how outspoken Dr. McCullough has been about the toxic nature of the lipid nanoparticles delivering mRNA, it is surprising that he didn’t mention on substack that this silent interfering RNA (siRNA) also gets delivered in a lipid nanoparticle (LNP) (although his paper certainly acknowledges their role).
Before I dive into the next bit, should you be interested…
Here is his post:

And here is mine:

👊 Now a friendly disclaimer… to go ahead and put your waders on.
We are headed out into the weeds.
PART 1: THE LIPID NANOPARTICLE
After warning for years about the hazards of the lipid nanoparticles (LNP) associated with the mRNA injections, in his substack post on 5/31/24, Dr. McCullough fails to mention that the siRNA used in the drug patisiran (which he is promoting) is also encapsulated in the infamous lipid nanoparticle technology👇.
Patisiran was developed and is marketed by Alnylam and uses lipid nanoparticles to deliver its payload. (source)
McCullough has been very vocal about the dangers of LNPs. A search of “lipid nanoparticle” on his stack returns the following results:
POSTS
Long-Lasting, Synthetic mRNA and Frameshifted Protein Products from COVID-19 Vaccination
Hematologic Abnormalities 90 Days after COVID-19 Vaccination
Arm Pain with COVID-19 Vaccination May be Key to Risk Stratification for Serious Complications
Lipid Nanoparticles Drive mRNA Delivery to Placenta and Hopefully no Further
…tic code. The synthetic mRNA carried on lipid nanoparticles appears to…
Potential Role of Spike Protein in Neurodegenerative Diseases
…ow abundant evidence that the synthetic lipid nanoparticles travel into …
The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review
…t al have published a scoping review of lipid nanoparticle-mRNA products with fair balance causing
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA
This vaccine is included in a lipid nanoparticle to be able to enter cells.
EVA Project Finds 78% of Women Report Menstrual Changes after COVID-19 Vaccination
Critical Role of Pseudouridine in Synthetic mRNA COVID-19 Vaccines
According to McCullough in this post, the LNP is uncontrollable and therefore has an unknown delivery location:
There is no control over where in the body the lipid nanoparticles will deliver the dangerous genetic payload. Additionally, all cells that take up mRNA express foreign proteins on the cell surface inviting an immediate auto-immune attack on cells harboring the mRNA and it’s protein products as described by Dr. Panagis Polykretis.
Here, McCullough describes LNPs as essentially being designed to interfere with humans’ reproductive systems.
Both forms of the vaccine use lipid nanoparticles which for years have been known to be taken up by reproductive glands (ovaries and testis) and dump their payload of genetic code…
Genetic vaccines loaded on lipid nanoparticles, are almost by design as depicted by Wang et al destined to influence ovulatory cycles, gametocyte production and viability, thus interfering with the complex and delicate reproductive cycle of human beings.
Historically McCullough seems to have been very concerned with the dangers of LNPs. However, in this endorsement of siRNA, he seems less so.
The two drugs he promotes share similar mechanisms of action and have the same target location. Both patisiran and inclisiran are RNA interference (siRNA) therapeutics focusing on gene silencing through the degradation of specific messenger RNA (mRNA) molecules.
They both use a LNP delivery system. Both drugs use this system to deliver siRNA to the liver. This is important because that’s what livers do; metabolize lipids (fat). So it’s reasonable to assume that LIPID nanoparticles will end up in the there, and if the payload is relevant to the liver (which it supposedly is in this case) it will be effective.
The mRNA from the covid injections however, is supposedly ending up everywhere, crossing the blood brain barrier, etc and wreaking havoc. Per McCullough, the distribution is uncontrolled and unpredictable.
This siRNA LNP must be different though! Maybe the future is brighter for LNPs!
McCullough concludes his endorsement of his own paper:
It may seem unfathomable for doctors to inject more RNA to deactivate Pfizer and Moderna synthetic mRNA that has accumulated in the body after multiple injections. However, siRNA used today in my practice (patisiran, inclisiran) appears to be safe and well-tolerated only notable for injection site reactions.
His recommendation seems to at least partially rest on his experience using siRNA technolgy (patisiran and inclisiran) in his practice.
I mean, the mRNA LNPs go everywhere but I’ve used these two siRNAs with LNPs that get taken up by the liver (doing what it does) and they seem to be “well tolerated”. So…
FIRE AWAY, the future’s brighter and stuff!!!
PART 2: THE DRUGS
Patisiran
Patisiran is sold under the brand name Onpattro. It was the first small interfering RNA-based drug to be approved by the U.S. Food and Drug Administration (FDA). It is a gene silencing drug that interferes with the production of an abnormal form of transthyretin. Patisiran was developed and is marketed by Alnylam and uses lipid nanoparticles to deliver its payload.
Formulation of the RNAi Agent Patisiran in Lipid Nanoparticle Carriers
The carrier used in patisiran is a second-generation lipid nanoparticle that contains combinations of synthetic ionizable lipid-like molecules known as lipidoids. This strategy was developed by Alnylam in collaboration with Dr. Robert Langer’s laboratory at MIT. The second-generation LNP renders patisiran much more potent than the first generation version of Alnylam’s anti-TTR product, ALN-TTR01.
Patisiran was granted orphan drug status, fast track designation, priority review and breakthrough therapy designation.
👆All of the above designations expedite approval and/or effect profitability.
Fast Track Designation must be requested by the drug company
Expedited review
FDA will reviews the request makes a decision within 60 days
👉 Orphan Drug designation includes the following:
Tax credits for qualified clinical trials
Exemption from user fees
Potential seven years of market exclusivity after approval
The per-patient cost for patisiran is between $451,430 and $677,145 per year, depending on the number of vials needed.
How Patisiran Came to Market
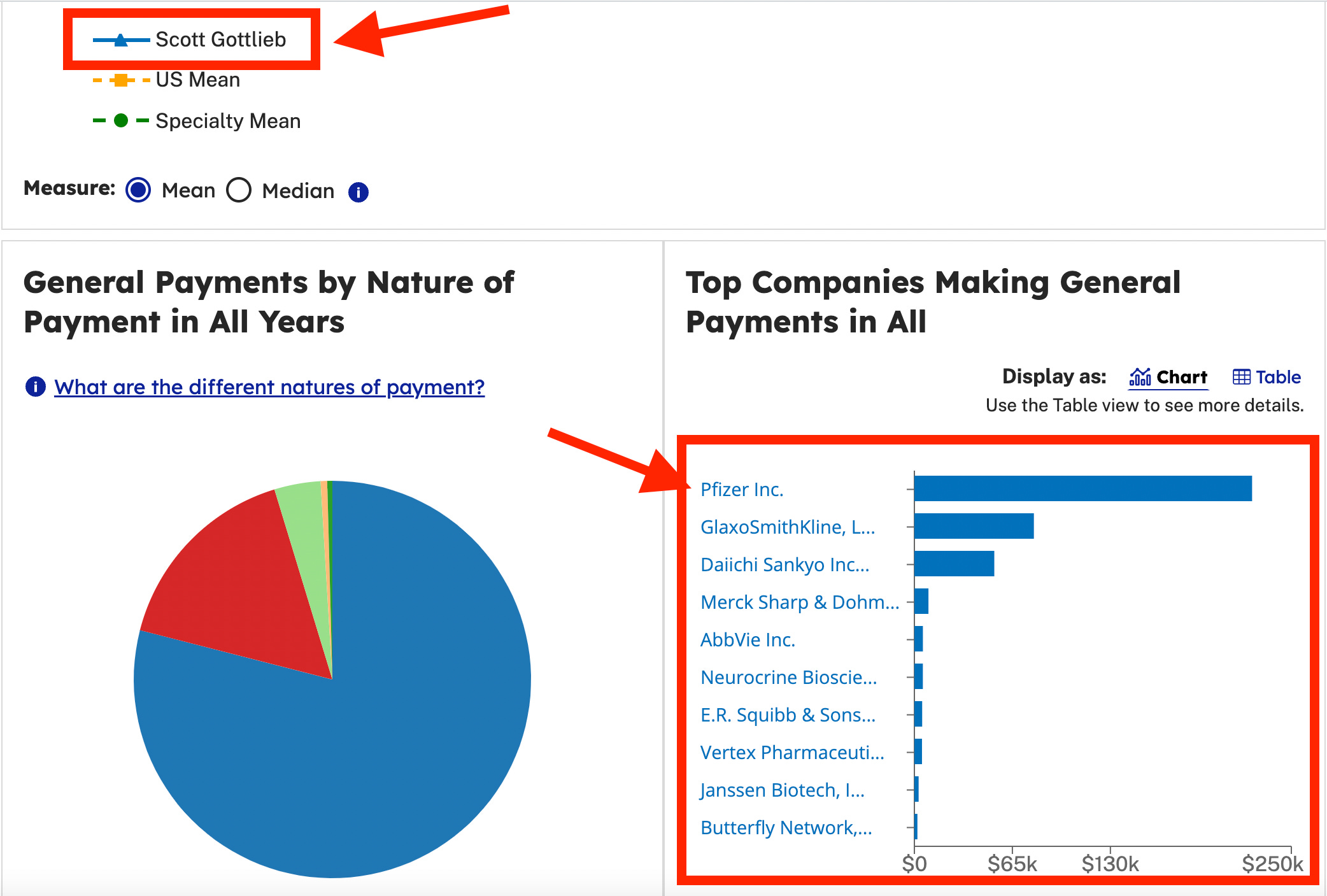
The clinical trial for patisiran was abundantly tainted by financial conflicts of interest (which I’ll address in a moment) and was the basis for granting expedited approval under FDA commissioner Scott Gottlieb. Gottlieb now sits on the board of another siRNA drug company, Comanche Biopharma.
FDA approves first-of-its kind targeted RNA-based therapy to treat a rare disease
FDA Commissioner Dr. Scott Gottlieb:
“New technologies like RNA inhibitors, that alter the genetic drivers of a disease, have the potential to transform medicine, so we can better confront and even cure debilitating illnesses.”
And if Scott Gottlieb’s on board, you know it’s good stuff! The former FDA Commissioner now reaps the rewards of his conflicting interests works in the industry.
I wrote about some of his recent interests here.

Gottlieb, who just happened to be the Commissioner of the FDA in 2018 when patisiran was fast tracked, has plenty of monetary incentives reasons to Fast Track an siRNA drug. Patisiran was approved just a few months before he resigned and now, he’s on the board of directors at Comanche Biopharma, a company specializing in…wait for it… siRNA.
What a coinkydink!
Let me be clear about why this part is a big deal. Approving a new (siRNA) technology essentially opens the door for subsequent approvals. Drug approval can be "piggybacked" on another similar drug through various regulatory pathways.
Moving on.
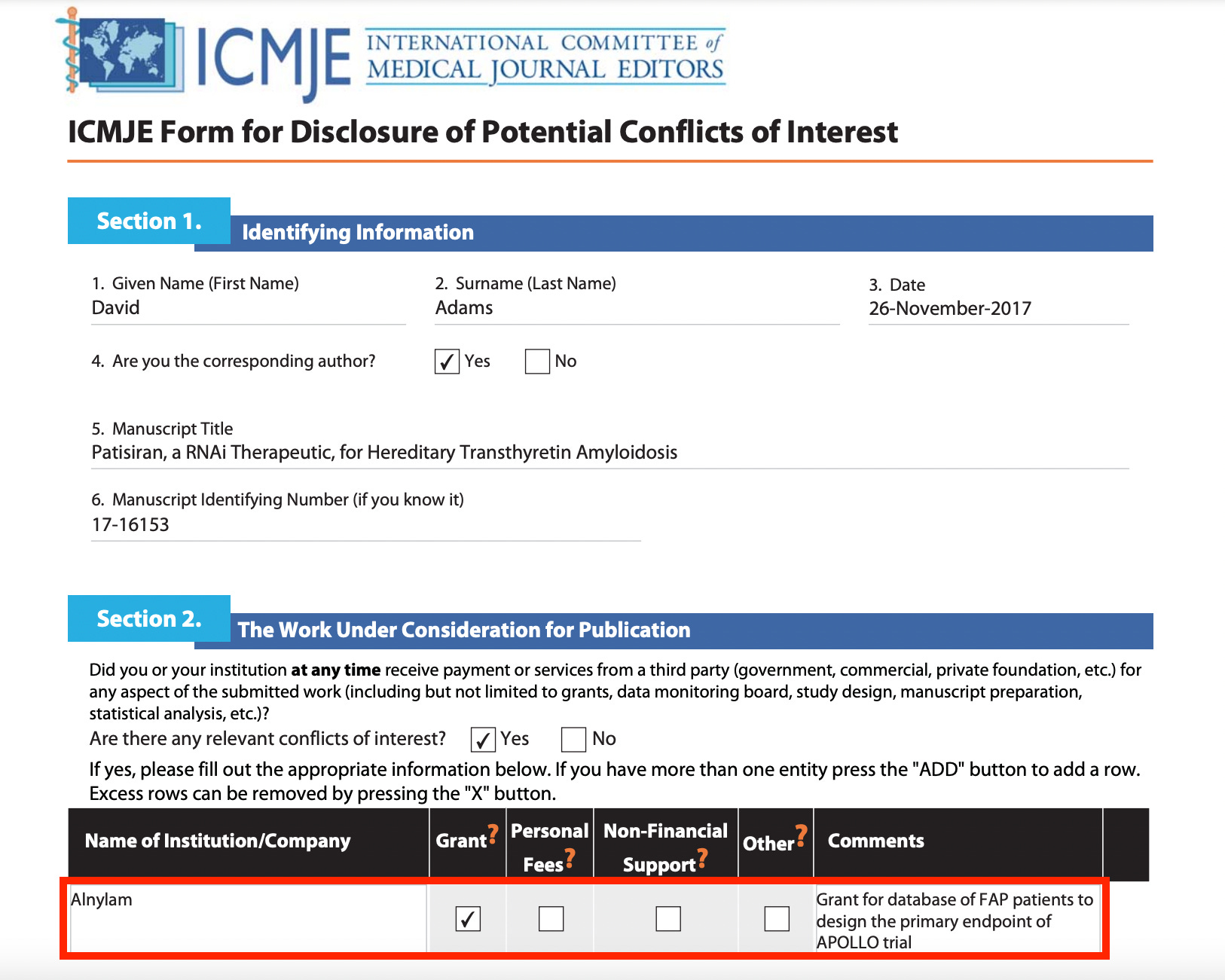
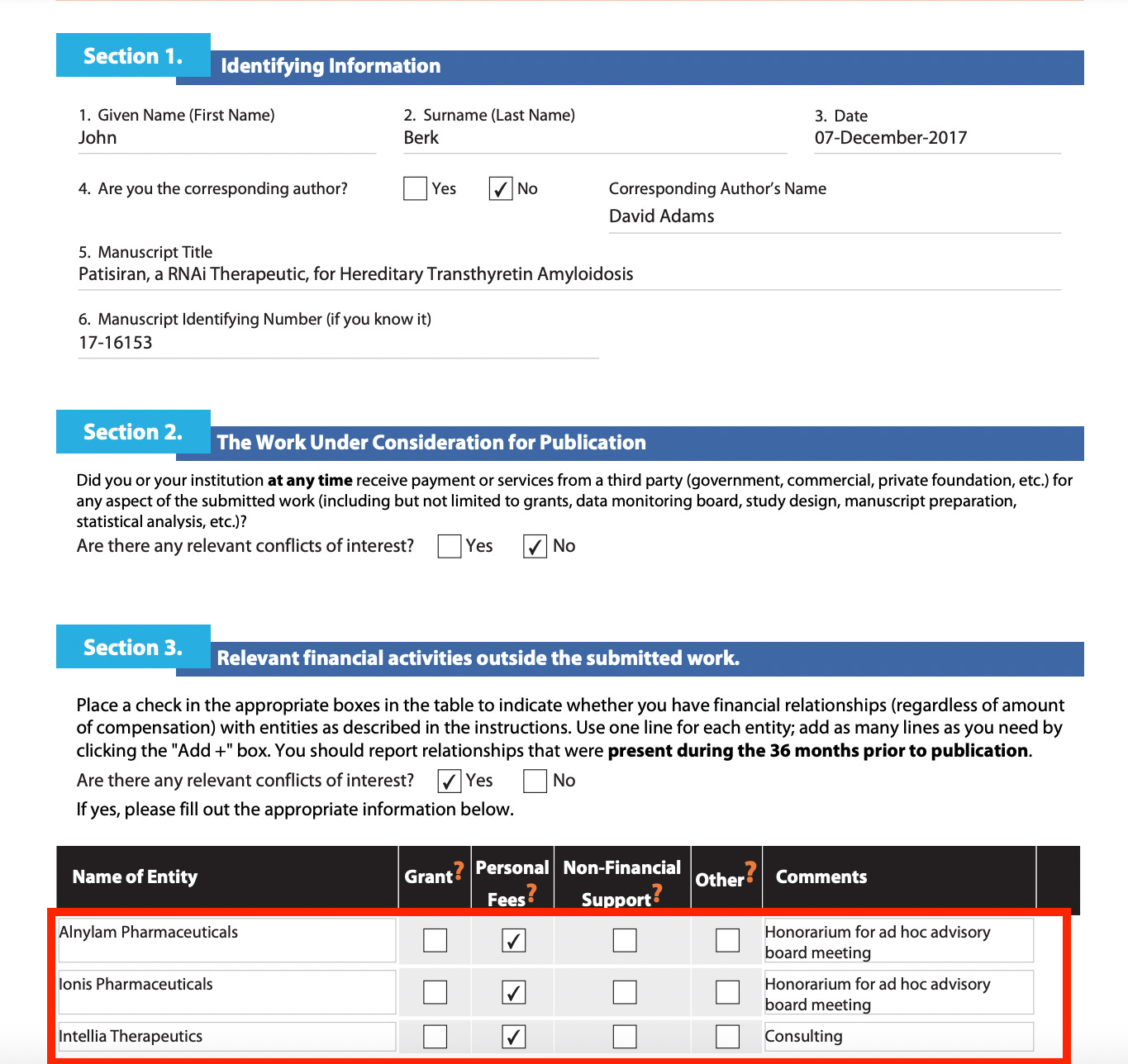
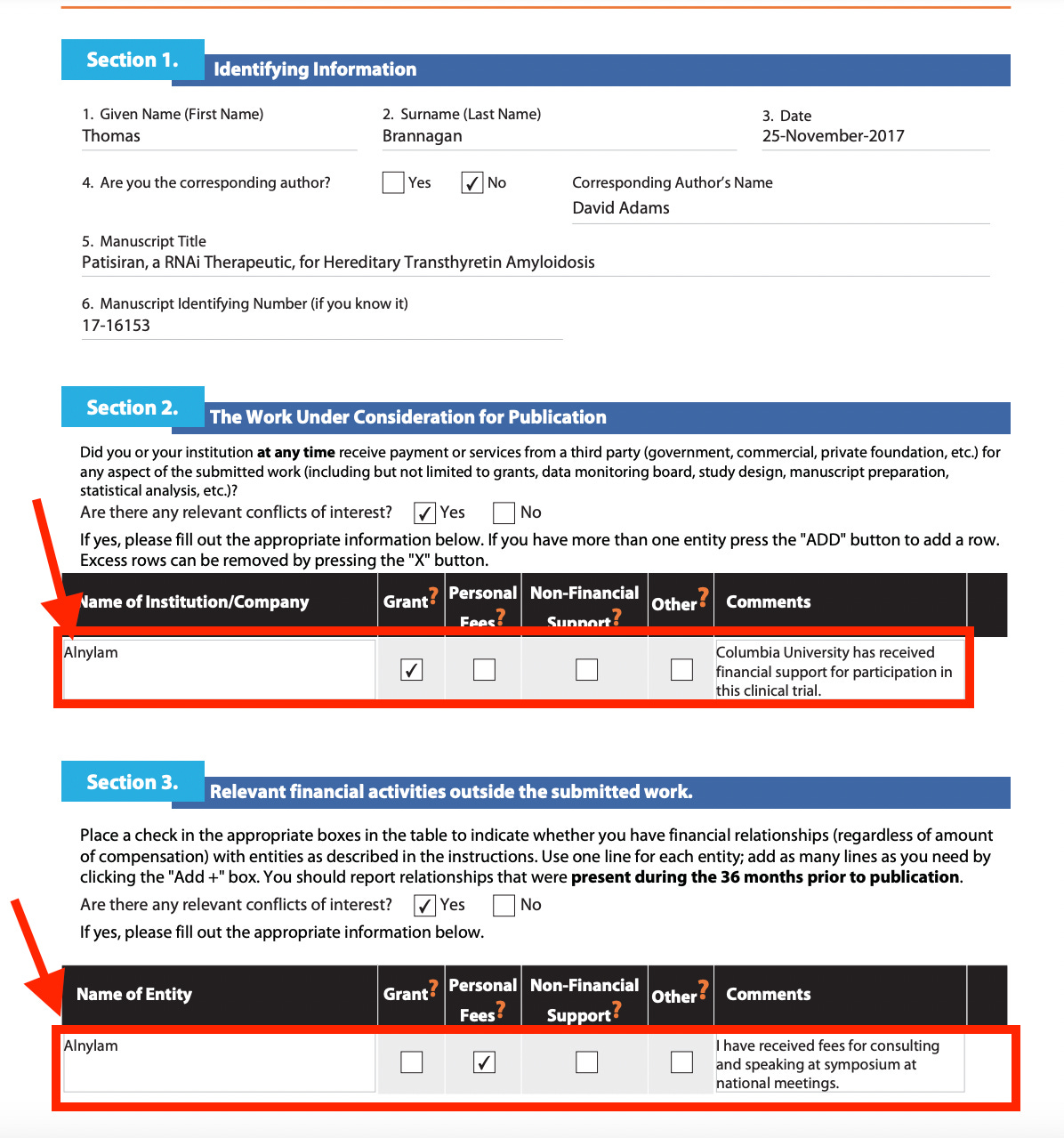
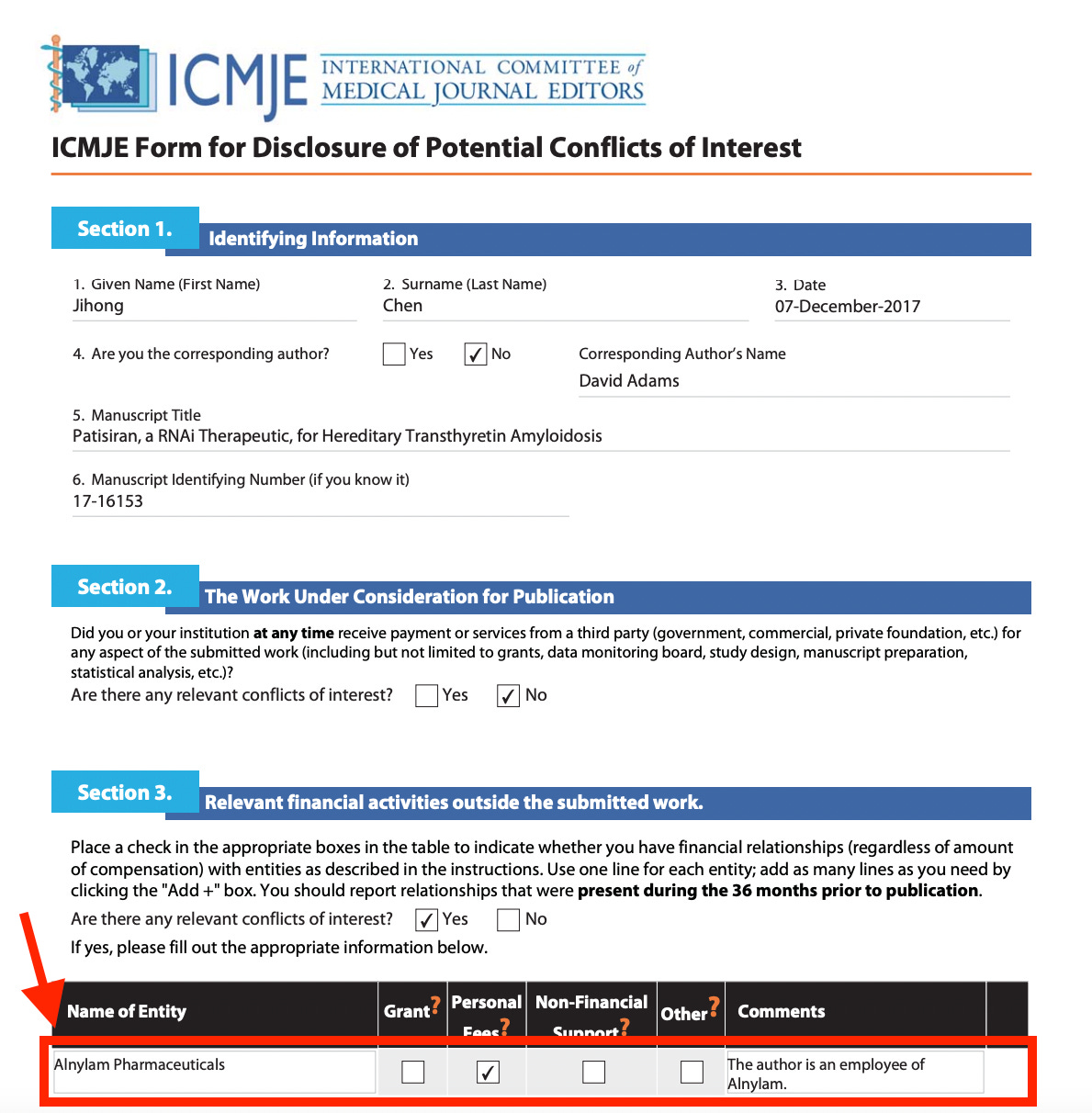
Let’s look at the clinical trial for patisiran.
There are 113 pages in the DISCLOSURES PDF. I didn’t go through and screenshot all of the conflicts of interest because…time. The majority of the conflicts of interest were with Alnylam, the company that makes patisiran.
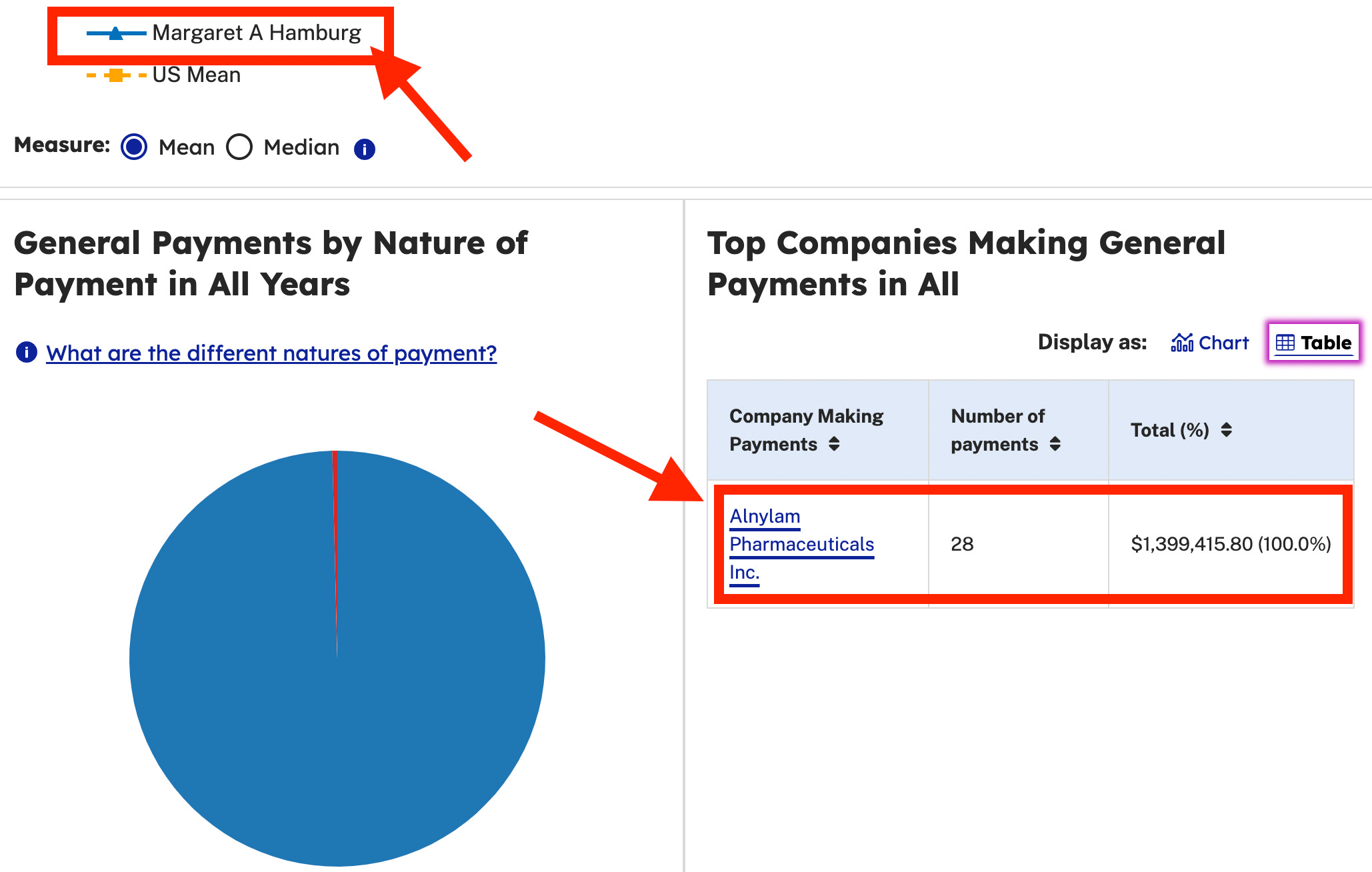
👉 Fun Fact: Former FDA Commissioner, Margaret Hamburg has received $1,399,415.80 from ALNYLAM since 2020 👈
Okie dokie.
Up next on McCullough’s reference list for why this siRNA injection strategy might be a good idea:
Inclisiran (Leqvio)
Inclisiran, is sold under the brand name Leqvio. It is an siRNA drug that interferes with RNA (genetic material) to limit the production of a protein that can increase levels of LDL-cholesterol. Leqvio was approved through New Drug Application (NDA) process based on clinical trial results.
FDA approves add-on therapy to lower cholesterol among certain high-risk adults
👇 THE FDA ON EFFECTIVENESS OF LOVQIO:
The effect of Leqvio on cardiovascular morbidity (suffering from a disease) and mortality (death) has not been determined.
The Clinical Trial Conflict of Interest Disclosures were unsurprisingly plentiful, and well-represented by many industry heavy hitters including…well, pretty much all of them.
Here is the statement:
Dr. Ray reports receiving lecture fees from Aegerion Pharmaceuticals, Kowa, Cipla, Algorithm, and Zuelling Pharma, grant support, paid to his institution, lecture fees, and advisory board fees from Amgen, Regeneron Pharmaceuticals/Sanofi, and Pfizer, lecture fees and fees for serving on steering committees for trials from AstraZeneca and Eli Lilly, fees for serving on steering committees for trials from Cerenis Therapeutics, the Medicines Company, and Esperion, advisory board fees from Akcea Therapeutics, Novartis, Silence Therapeutics, Bayer, and Daiichi Sankyo, lecture fees and advisory board fees from Takeda, Boehringer Ingelheim, and Dr. Reddy’s Laboratories, grant support and advisory board fees from Merck Sharp & Dohme, fees for serving on a clinical events adjudication committee from AbbVie, and fees for serving as principal investigator for a trial from Resverlogix; Dr. Wright, receiving advisory board fees from Sanofi and Regeneron Pharmaceuticals, consulting fees from Gilead Sciences, and fees for serving on a steering committee from AstraZeneca; Dr. Kallend, being employed by and holding stock options in the Medicines Company; Dr. Koenig, receiving consulting fees and lecture fees from AstraZeneca, consulting fees from Novartis, Pfizer, the Medicines Company, DalCor Pharmaceuticals, Kowa, Amgen, Corvidia Therapeutics, and Daiichi Sankyo, lecture fees from Berlin-Chemie and Sanofi, and grant support and provision of reagents from Singulex, Abbott, Roche Diagnostics, and Dr. Beckmann Pharma; Dr. Leiter, receiving grant support, paid to his institution, advisory board fees, and fees for CME from Amgen, Eli Lilly, and Regeneron Pharmaceuticals/Sanofi, fees for serving on a steering committee from Esperion, grant support, paid to his institution, and fees for serving on a steering committee from Kowa and the Medicines Company, advisory board fees and fees for CME from Merck, and advisory board fees from HLS Therapeutics; Dr. Raal, receiving advisory board fees and lecture fees from Amgen, Sanofi-Aventis, Regeneron Pharmaceuticals, and the Medicines Company; Ms. Bisch and Ms. Richardson, being employed by and holding shares and stock options in the Medicines Company; Dr. Jaros, receiving fees for providing statistical analysis for trials from the Medicines Company; Dr. Wijngaard, being employed by and holding shares and stock options in the Medicines Company; and Dr. Kastelein, receiving consulting fees from Akcea Therapeutics, AstraZeneca, CiVi Biopharma, Corvidia Therapeutics, CSL Behring, Daiichi Sankyo, Draupnir Bio, Esperion, Gemphire Therapeutics, Madrigal Pharmaceuticals, Matinas BioPharma, NorthSea Therapeutics, Novo Nordisk, Novartis, Regeneron Pharamaceuticals, REGENXBIO, Staten Biotechnology, and 89bio. No other potential conflict of interest relevant to this article was reported.
PART 3: YOU GET THE SCIENCE YOU PAY FOR
Why have I taken you all the way out in the weeds over two drugs that were off handedly mentioned on Peter McCullough’s substack? And why do I keep harping on this conflict of interest stuff?
It’s not just because the company that makes the drug is also funding the clinical trial. That’s the obvious part. And that’s certainly a piece of the fuckery…but it’s just a piece.
This little rabbit hole I’ve explored shows exactly how the sausage gets made.
A clinical trial is funded by a company that wants to sell the drug they are testing. If there is lucrative potential and/or necessity for regulatory pathway potential, it would be advantageous for other pharmaceutical companies to have staff on these trials and studies as well.
For example, in the case of siRNA, we have seen two drugs come to market. One came via expedited approval under an FDA commissioner that now stands to profit from the outcome of this approval. The second was approved through the standard New Drug Application process, based on clinical trial data. These trials were run with significant representation from a myriad of pharmaceutical companies.
This is important because once a drug or technology is approved, it provides the opportunity for others to be approved by piggy-backing on the original. If the original clinical trial outcomes were flawed (influenced by financial interests from the pharmaceutical industry), that flaw may never be corrected, and may serve as the foundation for subsequent drug approvals.
The process of gaining FDA approval by using existing data from a previously approved drug is officially called the 505(b)(2) New Drug Application (NDA). This regulatory pathway allows the applicant to rely in part on data not developed by the applicant, such as published literature or the FDA's findings of safety and efficacy for a previously approved drug.
This is why looking at disclosure statements matters. And it clearly shows why there is the notoriously revolving door between regulatory agencies and the industries which they regulate.

Scott Gottlieb, FDA Commissioner: 5/11/2017 - 4/5/2019
Margaret Hamburg, FDA Commissioner: 5/18/2009-4/6/2015

This is also how the vaccine industry operates and why there hasn’t ever been a true placebo controlled clinical trial. It’s why the product pipelines are all full of mRNA.
This is also how the medical device industry works.
And this is exactly why it matters to look at what a doctor is promoting under the guise of altruism, and who they have received funding from over the years.

I’ll leave you with these thoughts from John H:
This was an outstanding post, Sarah.
Some food for thought:
Dr PM is a clinician, not a basic science researcher. His subspecialty is non-interventional cardiology with a master’s degree in public health. He appears to have no actual working knowledge of molecular biology, drug or biological product design/development or in the laboratory setting. The payments documented here would therefore appear to be for the purpose of marketing potential or new products in his capacity as a well-recognized public medical spokesperson.
As far as I can ascertain, Dr PM has never addressed the plethora of reports from independent researchers who proved that there is only trivial (or none) amounts of nitrogen or phosphorus present in any of the 4 major CV19 “vaccines." That means there is likely minimal to no mRNA present in any of them, (if the vials studied are representative of the total universe of manufactured product). It is highly improbable on the basis of chance alone, that all the vials analyzed independently, would fail to contain nitrogen or phosphorus unless that was the intent. On the other hand, there are multiple substances in them which are toxic to humans. If I am wrong about any of these assertions, I am willing to amend my comments.
Then there is this:
If pathological viruses don’t exist (which seems increasingly likely), there can’t be any bird flu. In the unlikely circumstance that bird flu actually exists but can’t be diagnosed with PCR tests (PCR was proven to be an unreliable diagnostic test for CV19), bird flu can’t be diagnosed reliably. If that’s true, there is no medical indication for SiRNA’s or an mRNA “vaccine” for this alleged disease. The fundamental underlying assumptions upon which this new treatment is based, are either extremely doubtful or false. Anyone making such claims is at the least, highly suspect.
Moreover, when you see words/phrases like “seem effective", realize you are being subjected to propaganda since they are not valid medical or scientific terms. Recall that the CV19 "vaccines" were said to be "safe and effective" not seemingly so, and yet, they have been proven to be dangerous. It is wise to dismiss such efficacy claims entirely, unless and until they can be properly/independently verified. I am willing to reconsider any of the above assertions if presented with contrary/rigorous evidence.

Egas Moniz invented the prefrontal leukotomy (lobotomy) for treating mentally ill patients. For this he was awarded a Nobel Prize in 1949.
Always keep this in mind when dealing with doctors and scientists- especially those considered to be on the 'cutting edge.'
Pun intended.
Excellent post, Sarah. John H. nails it... The real "tell" in this "scientific breakthrough" is: "...siRNA used today in my practice (patisiran, inclisiran) APPEARS TO BE safe and well-tolerated only notable for injection site reactions."
This appears to me to indicate wishful thinking by would be scientists in search of a winning lottery ticket.
Until the "excess death" and "disability" numbers reflect the real-world toxicity of the LNP poisons there are BIG profits to be made, dontchaknow!