


Fake Pandemics. The Op and the Song.

Alrighty folks, I have really been thinking about how they’ve accomplished this thing.
I’m not the only one. Please see here, here, here, here, here, and here for others’ work on this matter.
I’m going to do my best to outline the playbook, and why this one had enough magic for a fake pandemic to sing and dance.
Media
Modeling
Falsified numbers(deaths)
PCR “testing”
Structural legal framework in place
Media
Here’s a video detailing how to handle advertising a fake pandemic that can easily be compared to the Covid response experienced in the United States.
Modeling
This is some early modeling bullshit a graph from the Imperial College, projecting the death and destruction of Covid-19 that helped shut down the world.

With some fascist fear porn lockdown recommendations.

In my opinion, the PCR “test” was the lynchpin to this entire operation, however before the PCR “test” could be fully exploited, the scary numbers had to be in place. This was accomplished by shocking numbers, amplified by blanket media coverage, in astonishingly few cities. For the purposes of this post, I will highlight the United States, specifically New York City.
Please see the following graph, from PANDA Uncut:

And now this graph from the CDC:

I am not going to cover the specific ways in which the numbers were made to be scary, however I encourage you to take the time to look into the immense amount of material available on PANDA-Uncut regarding this subject.
As far as faking a pandemic goes, the implications from the graphs above (augmented by the immense media coverage) were incredibly effective in creating the illusion of a pandemic.
In case you didn’t watch the entire video I included earlier…here’s a short clip of how this has already been done (40sec):
The mass casualty event had been established and was well advertised by every media outlet, amplifying “expert” reports from the hospital doctors…two of whom just happened to also be simulation experts (probably just a coincidence). For more insight on the distraught simulation expert physicians, see here and here.
The panic would be for naught without confirmation of a spreading pathogen though. Sooooo….
PCR “Testing”
In my opinion, the fake pandemic could not have been executed without the PCR fraud. Therefore, I believe that it is incredibly important to understand its role and how it was used…so that we understand how will be used to create situations that usurp our rights in the future.
Here are two key points:
PCR is the consumable that interacted with the most individuals overall (other than media, of course).
PCR “testing” is a conserved counter measure. Abundant testing persists, despite Covid falling into the background.
Just as we still take our shoes off at the airport, asymptomatic testing is a conserved countermeasure that has become widely integrated into societal behavior. I can tell you from daily experience in my studio that everyone is still testing all the time.
“We are going to see my aunt this weekend and she wanted us to test.”
“I had a headache this morning, it’s not Covid though, I tested.”
“I was a little stuffy and my doctor gave me a covid test at my annual checkup. I tested positive for Covid, but I feel totally fine.”
“I was having allergies, but I thought I should probably test anyway.”
“My kid is sick. It’s not Covid, flu, strep, or RSV, but I can’t come in today because he has a fever.”
I cannot overstate the importance of this piece. Society has become conditioned to test for any and everything. Or nothing. Relevant symptoms, unrelevant symptoms, no symptoms, by request…the list is endless.
The fake pandemic could not have been executed had asymptomatic testing (for supposed asymptomatic infection) not been a thing.
We can glean insight from reviewing the two prior coronaviruses that gained global attention; SARS-1 and MERS.
Why didn’t they rise to the celebrity status of SARS COV-2?
Enter PCR.
PCR is not new. It has been used for quite some time.
Here is inventor, Dr. Kerry Mullis:
PCR was used to “diagnose” both SARS-1 and MERS, however the PCR racket was amplified in significant ways that assisted Covid-19 in achieving its pandemic notoriety.
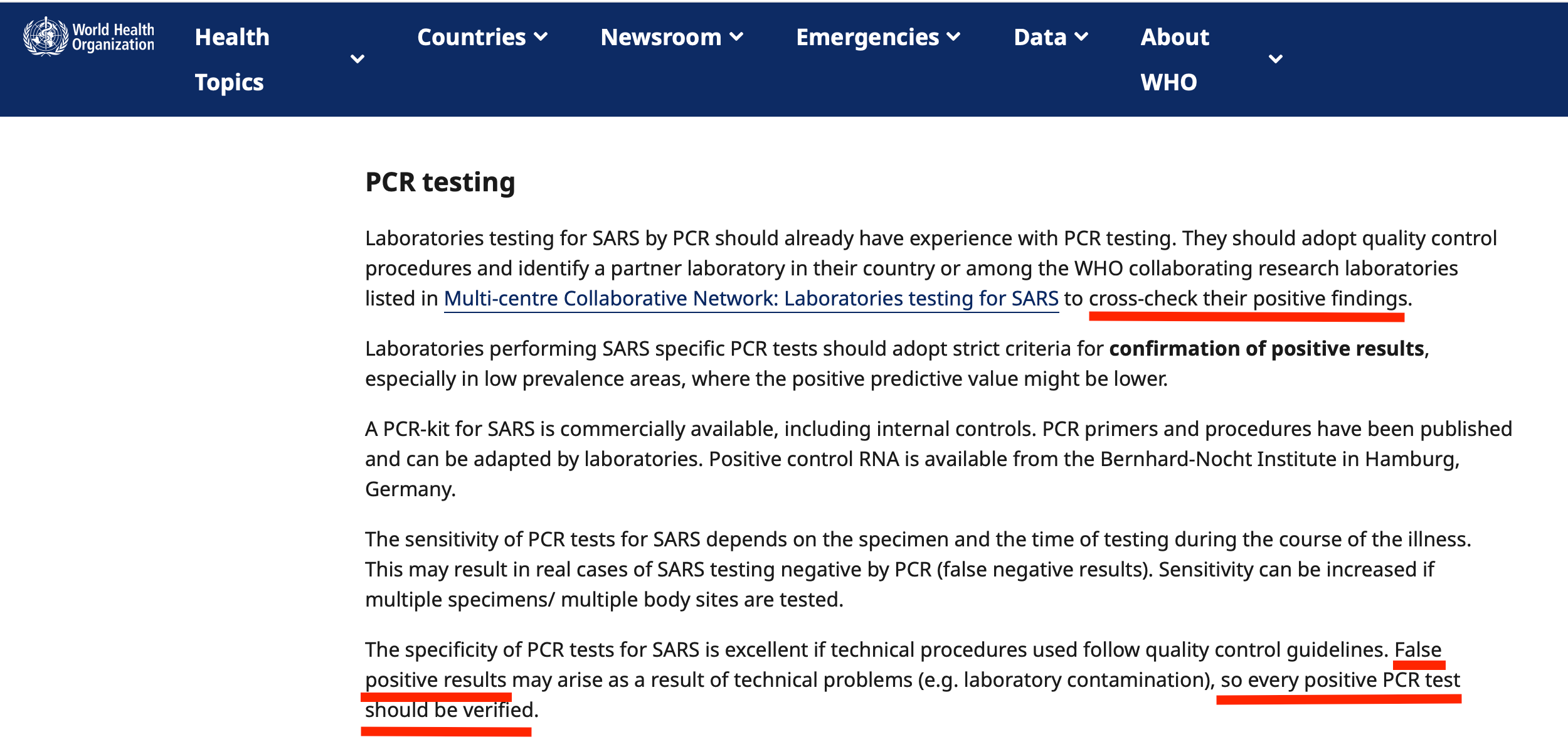
For example, SARS COV-1 guidance from the WHO encouraged cross checking findings and verifying “every positive PCR test”.
Can you imagine if this had been required for Covid??? They could never have pulled off the fake pandemic!
Use of laboratory methods for SARS diagnosis
2 May 2003
MERS also used the PCR, but simply didn’t have the get up and go that we’ve come to expect from a reliable coronavirus (the Covid-19 enchantment was different than MERS…consider JJ Couey’s work on how this was accomplished).
Fact Sheet for Health Care Providers: Interpreting RealStar® MERS-CoV RT-PCR Kit U.S. Test Results
February 12, 2016
The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) to authorize the use of the RealStar® MERS-CoV RT-PCR Kit U.S. for the in vitro qualitative detection of RNA from the Middle East Respiratory Syndrome Coronavirus (MERS- CoV).

So what did they learn from their failed pandemics???
Gosh, it sure would be easier to fake a pandemic if we could tell people they need to test even if they don’t have symptoms because they might be sick even though they aren’t sick.
💥BOOM💥
Enter
✨ ASYMPTOMATIC TESTING✨ + ✨ASYMPTOMATIC INFECTION ✨
This paper from 2021 describes the lynchpin:
Real-time PCR-based analyses combine the traditional PCR approaches and fluorescent-emitting compounds to measure the number of amplicons produced during the PCR amplification process in “real-time” [51]. By combining both real-time PCR and reverse transcription reaction, the gene expression level in the samples can be calculated [51]. With the introduction of qRT-PCR to detect both MERS-CoV and SARS-CoV, different health agencies and authorities like World Health Organization, US Food and Drug Administration (FDA), and US Centers for Disease Control and Prevention has sanctioned and revised the confirmed MERS and SARS-CoV-2 case definition in which individual who is tested positive for MERS-CoV or SARS-CoV-2 using qRT-PCR or serology test will be regarded as confirmed case, regardless of appearant clinical signs and symptoms.
…revised the confirmed MERS and SARS-CoV-2 case definition in which individual who is tested positive for MERS-CoV or SARS-CoV-2 using qRT-PCR or serology test will be regarded as confirmed case, regardless of appearant clinical signs and symptoms.
Mini review: Recent progress in RT-LAMP enabled COVID-19 detection
Conclusion and future trends
Rapid, low-cost, and user-friendly molecular diagnostic methods are prerequisite to address the outbreaks of infectious diseases. Especially during the outbreak of COVID-19 pandemic, there is an urgent need to build the global testing capacity up to 100-fold above what is achievable with current standard approaches [19]. LAMP is an innovative gene amplification technique that shows great promise as a detection tool, especially during this coronavirus pandemic. Here, we summarize recent progress in the RT-LAMP assays for rapid and accurate detection of SARS-CoV-2 nucleic acids. Even though false results are still present, the advantages of using the LAMP process are still immense. One major benefit is the speed of the analysis, as the confirmation of results for the typical RT-LAMP procedure is faster than that of the RT-PCR, by a wide margin.
If you have any doubt about the staying power of PCR in the fake pandemic business model…
The global digital pcr market was valued at $508.82 million in 2020, and is projected to reach $1,305.30 million by 2030, growing at a CAGR of 8.6% from 2021 to 2030. (source)
There are many companies that are conveniently well positioned to offer the next generation of testing. At home diagnostics “that will create a significant impact”. Because Zev.
Nanobiosym’s Gene-Radar has been applied to various diagnostic applications, including the detection of infectious diseases such as COVID-19, HIV/AIDS, tuberculosis, and Ebola virus disease. The platform's versatility and adaptability make it a valuable tool for addressing public health challenges and improving healthcare delivery worldwide.
Gene-RADAR® harnesses over 20 years of research at the frontier of nanobiophysics to enable the world’s first, mobile, Tricorder device that enables gold standard real-time diagnosis of any disease with a genetic fingerprint; at a cost at least 10 times cheaper than any comparable diagnostic tests on the market today.
“The Ebola global crisis was a teachable moment for just how interconnected we all are and indeed just how vulnerable our planet is to pandemic threats,” said Dr. Goel. “What Google did for access to information, and the iPhone did for telecommunications, we at Nanobiosym are doing for healthcare. We are decentralizing, personalizing, and mobilizing the next generation of healthcare. Our Gene-RADAR literally puts Your Health in Your Hands™. (source)
Just a reminder…PCR is used to test your wastewater, which is yet another way you can be told that you are sick.


Structural Legal Framework
Please see the extensive work of Katherine Watt for detailed explanation of this mechanism. I’ve written several posts, all based on Katherine’s work, regarding the legal framework that was, and is, in place allowing fake pandemics to take place… and more importantly the bioweapon countermeasures to be deployed upon the citizens of the world (one of which was PCR“test”).
I won’t rehash the work I linked above, however I would like you to consider a few historical events and their subsequent effects, through a pandemic lens.
The terrorist attacks on September 11, 2001, prompted significant changes in airport security worldwide. In response to the events of 9/11, various measures were implemented to enhance aviation security and prevent similar attacks in the future. Here are some of the key changes that occurred in airport security following 9/11:
Creation of the Transportation Security Administration (TSA): The TSA was established by the U.S. Congress in November 2001 as part of the Aviation and Transportation Security Act. The TSA is responsible for overseeing security screening at airports in the United States and implementing measures to protect the nation's transportation systems.
Federalization of Airport Security Screening: Prior to 9/11, airport security screening in the United States was primarily conducted by private companies under the oversight of airlines. Following the attacks, security screening responsibilities were federalized, and the TSA assumed direct responsibility for conducting passenger and baggage screening at U.S. airports.
Implementation of Passenger Screening Measures: Airport security screening procedures were significantly enhanced, with the introduction of measures such as passenger screening checkpoints, metal detectors, X-ray machines for carry-on baggage, and explosive detection systems. These measures were designed to detect and prevent the smuggling of weapons and explosives onto aircraft.
Introduction of Prohibited Items List: The TSA implemented a list of prohibited items that are not allowed in carry-on baggage, including firearms, knives, box cutters, and other potential weapons. This list has been periodically updated to address emerging security threats and enhance aviation security.
Increased Scrutiny of Passengers and Baggage: Passengers and their baggage underwent more rigorous screening procedures, including thorough checks for prohibited items and potential security threats. Enhanced screening measures, such as random secondary screenings and behavioral observation techniques, were also implemented to identify individuals exhibiting suspicious behavior.
Enhanced Intelligence Sharing and Coordination: Improved coordination and information sharing between government agencies, law enforcement agencies, and international partners were prioritized to strengthen aviation security and prevent terrorist attacks.
Do you remember why we take our shoes off when going through airport security?
The requirement for passengers to remove their shoes as part of airport security screening became more widespread following the attempted shoe bombing incident on December 22, 2001. In this incident, one Richard Reid, also known as the "Shoe Bomber," attempted to detonate explosives concealed in his shoes on American Airlines Flight 63 from Paris to Miami.
Following the attempted attack, security measures at airports were significantly enhanced, and shoe removal became a standard practice in security screening procedures at airports around the world. The Transportation Security Administration (TSA) in the United States implemented the requirement for passengers to remove their shoes for X-ray screening as part of heightened security measures aimed at preventing similar threats.
What about liquids? Do you remember why we dump our water out and have to carry all those small bottles of shampoo?
The restrictions on carrying liquids through airport security checkpoints were implemented following the foiled "liquid bomb plot" in August 2006. This plot involved a plan to detonate liquid explosives on multiple transatlantic flights departing from the United Kingdom to the United States and Canada.
These changes have been integrated and accepted into habitual societal behavior.
There are many artifacts of Covid that remain…and that are unfortunately being normalized. PCR testing is one of the most relevant when considering “the next pandemic”, which is being advertised on every front, and will likely be faked in very similar ways.
If you made it this far, thank you 😂… I wish I were better at SUCCINCT. But I’m not.
Here is the new hit, “Fake Pandemics”, for your listening pleasure.
Stay tuned for the remix.
Sarah, thank you for this. I agree 100% that fake PCR "tests" are the lynchpin. Serology-based antigen and antibody "testing", also. I have spent SO. MUCH. TIME. over the past 4 years telling co-workers, family, friends, and total strangers that the tests are absolutely meaningless BS. Even people who have awareness of the truth re: the “pandemic” still believe the results are credible. I highly recommend PANDA, as well. It was data analyses and other information from PANDA in 2020 that really opened my eyes to what was actually going on.
As a medical laboratory scientist employed in hospital labs, forced to perform rapid NAAT methodologies to “diagnose” SARS-CoV-2 for more than 2 years, I was stressed to the point of breaking. Performing those tests meant I was helping to falsely elevate “covid” case numbers, and if any of the patients with a worthless “positive” result died for any reason whatsoever, the COD would be “covid.”
Adding to my frustration and anger was the fact that none of my colleagues - most of whom had also studied and performed PCR and other NAAT methodologies - seemed to grasp why it was a misapplication of the technology. I was constantly talking about the non-diagnostic nature of PCR, not to mention the high threshold cycles being used. I was met with blank stares or shrugs every time I pointed out that Ct (threshold cycle) is inversely proportional to viral load. Or that finding the target nucleic acid sequence (if that is what the primers were even designed for) in the sample and then amplifying it to detectable levels is not synonymous with infection. Even though I did not trust the WHO at the time, I pointed to the guidance for medical professionals issued in early 2021 urging providers to consider PCR "results" in the context of signs and symptoms, as well as cautioning against high threshold cycles. It was only half-truths, but I figured if the WHO was saying even this much, maybe I could get people's attention. (I read the guidance on the WHO website, but can no longer find it. It was probably memory-holed. They also said very early on that asymptomatic presentation of respiratory viral infections is extremely rare, before completely backtracking and flip-flopping. No one remembers that bit, do they?) No matter what I pointed out, my colleagues were all convinced of the validity of the results.
Some nights I was so overwhelmed by the volume of samples I’d receive for fake testing that my anger would overflow and I’d start throwing the specimen vials across the lab. The stress from early 2020 through Fall of 2021 was destroying me on every level.
Then I could no longer practice my profession in NY, because I refused to be injected. On very short notice, I found a job in another state and relocated 1,000+ miles from home, family, and friends in the hope that I could remain employed, though I had no guarantees regarding mandates. (Shortly after arriving in my new state of residence, the CMS "vaccine" mandate came down, affecting everyone in healthcare throughout the country. Then I had to play the exemption game, but I did not even have that option in NY.) The first two hospital systems I worked for also compelled me to do "covid testing", but I could not afford to lose another job, especially now that I lived someplace I had never been to before, and where I knew no one. I cried pretty much every day and lost a lot of sleep, because I was part of it all, even though it was unwillingly.
That was only a part of the ordeal, however. I can’t describe the anguish I felt as a blood banker, knowing I was facilitating the transfusion of tainted blood to those who chose not to be injected. Transfusion services was my passion, and I had a job offer to work exclusively in the blood bank at Mayo Clinic, but my offer was withdrawn when I refused, once again, to be injected with a deadly, gene-altering bioweapon. It was a blessing in disguise, though, because I could not have continued as a blood banker with a clear conscience. I also know now that Mayo, like other large healthcare systems, is extremely DEI/ESG. I spoke with a lawyer who had successfully sued Mayo to get alternative treatments for patients with a covid diagnosis. He said Mayo was using the shot mandate to weed out conservative - or dissident - individuals. And, like pretty much all of "healthcare" now, they are deeply invested in the disgusting profitability of "covid."
In late 2022, I finally found employment that requires neither “covid testing” nor blood banking so I don’t disintegrate from the unbearable strain of helping perpetuate the deadly deception. I have changed jobs 3 times in 2.5 years, not including the withdrawal of Mayo's job offer. Since I work in a captured "industry" I am mostly surrounded by the duped. With less job stress, I am able to focus more on getting real data and factual information to colleagues. Most days, it's still an uphill battle, but I can't stop fighting. I don't know if I'll ever be free of the guilt I feel for having been part of the machine for as long as I was.
UWB (ultrawide band radiation) can track our location down to less than 30 centimeters/ 1 foot.
That's why ditching our phones is the first step to not being on the gene radar, at least it can't hurt:
https://romanshapoval.substack.com/i/140673931/iphone-implants