

Have you noticed a lot of people are sick with "not covid"?
There's no reason anyone should be surprised. *apologies in advance for the lengthy article*

I have been citing Geert Vanden Bossche for years now (years…I still can’t believe that we are 3 years into this fuckery).
He either has a functional crystal ball or he knows wtf he’s talking about because he has been right. A lot. Check him out HERE, HERE, and HERE.
I wonder if he’s being showered with humble apologies from all of those “experts” that so unceremoniously refuted his warnings?
I bet Jonathan Jarry M.Sc. is going to follow up on his article from March of 2021 (with the condescending tag pseudoscience) where he said,
Dr. Bossche makes a number of incorrect or exaggerated claims about the use of mass vaccination during a pandemic and urges international health authorities to stop the current crop of COVID-19 vaccines or else risk unleashing “a global catastrophe without equal.” This is scary stuff, but it’s all quite misguided…
“But if you have a vaccine that results in high levels of neutralizing antibodies, that’s not a way to create variants,” he [Paul Offit] continued. To use an analogy, if a gaggle of invaders is coming but you have only managed to round up a few soldiers, be prepared for a long siege during which the enemy might learn a thing or two about your defences and adapt. But if you have a full and overpowering army at your command, the invaders won’t stick around for long. So the question becomes: do the COVID-19 vaccines give us low or high levels of neutralizing antibodies?
While scientists don’t yet know exactly what levels of antibodies are needed to ward off disease, the approved vaccines do elicit the production of neutralizing antibodies.

Geert has LOUDLY protested broadly vaccinating the population during a pandemic. You can take a look HERE.
He told us that this vaccine strategy would result in an increase in other respiratory infections…much like we are seeing now.

As I’ve mentioned before, I hold zero authority to speak on these topics, which is an excellent reason for you to do your due diligence and check all of this for yourself. I’ve included a large portion of Dr. Vanden Bossche’s most recent article below. To read the article in its entirety click HERE.
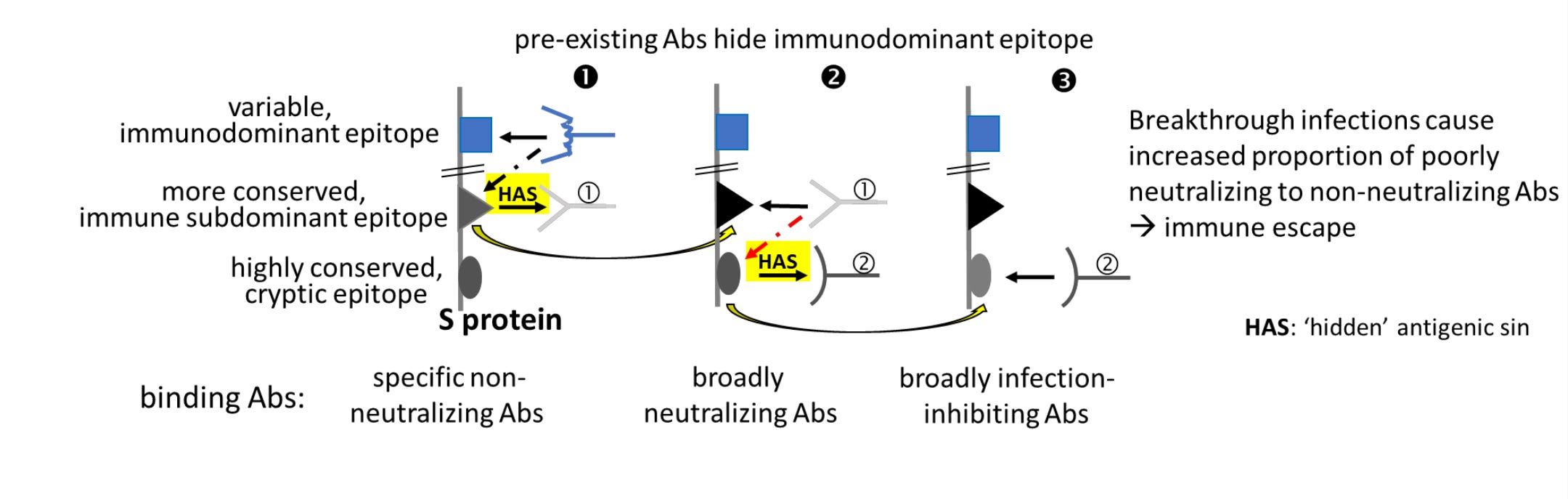
If you would prefer to watch, Dr. Vanden Bossche explains his slide below and the concept of immune refocusing and ‘hidden’ antigenic sin in this VIDEO.
But first…
Surprisingly, I didn’t learn much about virology and immunology when I was getting my dance degree; so I’ve had to do a little additional reading to even entertain the idea of understanding anything Geert publishes. If you don’t have a background in this arena, you might find it helpful to peruse the following:
Antigen
In general, antigens are composed of proteins, peptides, and polysaccharides. Any portion of bacteria or viruses, such as surface protein, coat, capsule, toxins, and cell wall, can serve as antigens.
An antigen contains distinct sites on its surface, called an epitope or antigenic determinant. Antibodies generated against an antigen recognize and interact with specific epitopes via antigen-binding sites (paratopes) to trigger immune responses.
Epitope
An epitope is the part of an antigen that the host’s immune system recognizes, eliciting the immune response to an invading pathogen. It specifically binds to the corresponding antigen receptor on the immune cell (such as a B cell) and binding only occurs if the structures are complementary.
Once epitope and receptor bind together in this puzzle-like combination, the production of antibodies is stimulated. These antibodies are specifically targeted to the epitopes that bind to the antigen receptors. In this manner, the epitope is also the region of the antigen that is recognized by the specific antibody which then removes the antigen from the host organism after binding to it. The region on the antibody which binds to the epitope is known as the paratope.
Many antigens have a number of distinct epitopes on their surfaces. Each of these epitopes can interact with different antigen receptors on immune cells. The blood serum of an immunized person usually contains a mixture of antibodies that can bind with different epitopes on the surface of an antigen. Antibodies that target with the same epitope can have different abilities to bond with it.
Receptor Biding Domain
A receptor-binding domain (RBD) is a key part of a virus located on its ‘spike’ domain that allows it to dock to body receptors to gain entry into cells and lead to infection. These are also the primary targets in the prevention and treatment of viral infections, including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) – the virus that causes COVID-19.




A neutralizing antibody (NAb) is an antibody that defends a cell from a pathogen or infectious particle by neutralizing any effect it has biologically. Neutralization renders the particle no longer infectious or pathogenic.[3][4] Neutralizing antibodies are part of the humoral response of the adaptive immune system against viruses, intracellular bacteria and microbial toxin. By binding specifically to surface structures (antigen) on an infectious particle, neutralizing antibodies prevent the particle from interacting with its host cells it might infect and destroy.
Difference between neutralizing antibodies and binding antibodies (emphasis is mine)
Not all antibodies that bind a pathogenic particle are neutralizing. Non-neutralizing antibodies, or binding antibodies, bind specifically to the pathogen, but do not interfere with their infectivity. That might be because they do not bind to the right region. Non-neutralizing antibodies can be important to flag the particle for immune cells, signaling that it has been targeted, after which the particle is processed and consequently destroyed by recruited immune cells.[9] Neutralizing antibodies on the other hand can neutralize the biological effects of the antigen without a need for immune cells. In some cases, non-neutralizing antibodies or insufficient amounts of neutralizing antibodies binding to virus particles can be utilized by some virus species to facilitate uptake into their host cells. This mechanism is known as antibody-dependent enhancement.[10] It has been observed for Dengue virus and Zika virus.[11]
Antibody-dependent enhancement (ADE), sometimes less precisely called immune enhancement or disease enhancement, is a phenomenon in which binding of a virus to suboptimal antibodies enhances its entry into host cells, followed by its replication.[1][2] The suboptimal antibodies can result from natural infection or from vaccination. ADE may cause enhanced respiratory disease, but is not limited to respiratory disease.[3] It has been observed in HIV, RSV virus and Dengue virus and is monitored for in vaccine development.[4]
In ADE, antiviral antibodies promote viral infection of target immune cells by exploiting the phagocytic FcγR or complement pathway.[5] After interaction with a virus, the antibodies bind Fc receptors (FcR) expressed on certain immune cells or complement proteins. FcγRs bind antibodies via their fragment crystallizable region (Fc).
The process of phagocytosis is accompanied by virus degradation, but if the virus is not neutralized (either due to low affinity binding or targeting to a non-neutralizing epitope), antibody binding may result in virus escape and, therefore, more severe infection. Thus, phagocytosis can cause viral replication and the subsequent death of immune cells. Essentially, the virus “deceives” the process of phagocytosis of immune cells and uses the host's antibodies as a Trojan horse.
ADE may occur because of the non-neutralizing characteristic of an antibody, which binds viral epitopes other than those involved in host-cell attachment and entry. It may also happen when antibodies are present at sub-neutralizing concentrations (yielding occupancies on viral epitopes below the threshold for neutralization),[6][7] or when the strength of antibody-antigen interaction is below a certain threshold.[8][9] This phenomenon can lead to increased viral infectivity and virulence.
ADE can occur during the development of a primary or secondary viral infection, as well as with a virus challenge after vaccination.[1][10][11] It has been observed mainly with positive-strand RNA viruses, including flaviviruses such as dengue, yellow fever, and Zika;[12][13][14] alpha- and betacoronaviruses;[15] orthomyxoviruses such as influenza;[16] retroviruses such as HIV;[17][18][19] and orthopneumoviruses such as RSV.[20][21][22] The viruses that cause it frequently share common features such as antigenic diversity, replication ability, or ability to establish persistence in immune cells.[1]
The mechanism that involves phagocytosis of immune complexes via the FcγRII/CD32 receptor is better understood compared to the complement receptor pathway.[23][24][25] Cells that express this receptor are represented by monocytes, macrophages, and some categories of dendritic cells and B-cells. ADE is mainly mediated by IgG antibodies,[24] but IgM[26] and IgA antibodies[18][19] have also been shown to trigger it.
Dr. VDB presents immune refocusing as the mechanism that’s at work here. He didn’t make up immune refocusing. It’s a thing. Deceptive imprinting and immune refocusing in vaccine design was published in 2004. This study from 2008 addressed the topic as well:
A large number of pathogens appear to exploit this weakness in the host immune system by focusing antigenic attention upon highly variable epitopes while avoiding surveillance toward more highly conserved receptor binding sites or other essential functional domains. Because the propensity of the immune system to react against immunodominant strain-specific epitopes appears to be genetically hard-wired, the phenomenon has been termed “deceptive imprinting.” In this review, the authors describe observations related to deceptive imprinting in multiple systems and propose strategies for overcoming this phenomenon in the design of vaccines capable of inducing protection against highly variable pathogens
Summary and conclusions
The difficulties surrounding the design of broadly protective vaccines against Class II pathogens suggest that novel approaches are needed in research and development efforts. In the past few decades, it has become very clear that increasing the magnitude of immune responses with multiple boosts, larger quantities of immunogen, novel vector systems, or more stimulatory adjuvants will continue to fall short in meeting the demands for vaccines against many of the world’s most important pathogens.
Here’s his slide (again) illustrating the process:
We are able to see this happening in real time. Remember when the vaccines were 100% effective against infection and transmission? Then they couldn’t prevent transmission or infection BUT they prevented severe disease (#I just tested positive for covid #I’m so grateful for a mild infection thanks to my vaccine).
So what’s next? It’s not rocket science. Let’s check in with the experts…
Edward Nirenberg (interesting name) had this to offer up this time last year:
His claims are speculative, he offers no evidence to support his arguments, and makes several comments which are blatantly incorrect. The core of his argument relies on the assumption that COVID-19 vaccines do not have a significant effect on transmission. This has been repeatedly confirmed to be false in multiple studies.
Oops, Edward.
It appears that the jabs don’t have any significant effect on transmission, despite all those studies.
Hopefully Geert is wrong. But so far, he’s been spot on.
Next up → full immune escape → severe disease
NEW DATA SHOWS TROUBLING TREND IN VACCINATED
Data Reveals Higher Covid Rate in the Vaccinated
The Pandemic of the Vaccinated is Here
Hmmm…..
I’ll let Dr. VDB explain it now. The following is copied directly from Dr. Vanden Bossche’s article on his website:

On rare occasions I read some vaccine talk produced by mainstream journalists. It is interesting to see how in light of the continuing series of disappointing vaccine experiments on humans they cautiously begin to balance their remaining critical thinking faculties with the mainstream narrative that dominated their views for so long. The recent article: ‘Updated Covid-19 vaccines boost protection, but may not beat original formula against BA.4 and BA.5, early studies suggest ‘ is one such marvelous example.(https://edition.cnn.com/2022/10/26/health/updated-boosters-omicron-imprint/index.html)
Since I am much better at mastering the science than I am the language, I am going to provide science-based critiques to the big gaps in the immunological interpretation of the data reported on the first bivalent booster studies. I’ll share my comments to the cited interpretations of leading scientists and experts, however I’ll refrain from citing their names as I have no intention to ridicule these individuals—I only intend to point out the immunological ignorance of those still officially referred to as acknowledged key opinion leaders and decision makers in the field. Their immunological ignorance is now inspiring further efforts to fight evil (mass vaccination) with more evil (mass vaccination with updated vaccines)—a recipe for disaster that will certainly end the pandemic the ‘hard’ way. Nature will ultimately teach them how immunology works, and unfortunately not before massive damage is inflicted by the mass vaccination experiment. Before I get to the specific comments uttered by our leading ‘experts’ and cited within this article, I’ll open with a mind-boggling statement made by the journalist to first give a “masterclass” of softs in immunology to these very leading ‘experts’:
“But the hope was that by tweaking the vaccine recipe to include currently circulating strains of theOmicron variant, it would help broaden immunity against those variants and perhaps offer better and longer-lasting protection”
Geert (G): How can one conduct experiments on humans just based on some naïve ‘hope’? Why do scientists produce extensive data on deep mutational scanning without investigating the immunological driver behind the patterns of such reported mutations? If they would only do so, they would immediately realize the abundance of scientific rationale that could substitute for all the hope they put in empirical research on humans.
The scientific evidence clearly indicates that no single updated/ adapted vaccine booster will improve the temporary protective effect conferred by the Wuhan-Hu S-based C-19 vaccines but will instead only expedite immune escape.
Why?
Meanwhile, a myriad of reports documenting the convergent mutations in steadily evolving SARS-CoV-2(SC-2) variants unambiguously illustrates that both productive vaccine breakthrough infections and mRNA vaccine-based boosters place immune pressure on more conserved, immune subdominant spike (S)-associated epitopes by recalling immature memory B cells that produce low affinity antibodies (Abs).Of course, the resulting suboptimal pressure exerted by these Abs on these more conserved antigenic domains drives immune escape, first away from the recalled broadly neutralizing (i.e., variant-nonspecific) Abs and subsequently from the broadly infection-inhibiting Abs. This is due to ‘immune refocusing’, a phenomenon that occurs when pre-existing Abs bind to their pathogen-associated target epitopes with low affinity (i.e., not allowing virus neutralization in case of SC-2, for example): see fig.attached at the bottom. In this way, previously immunodominant epitopes expressed on the free-circulating antigen (e.g., spike protein in case of SC-2) can no longer be recognized by the host immune system whereas previously outcompeted antigenic determinants comprised within the same antigen but expressed on infected or transfected target cells will take advantage of the masking effect to recall the corresponding previously primed Abs.
The existence of previously primed ‘mismatching’ Abs is quite obvious in case of breakthrough infections, but how does this occur in case of mRNA booster vaccines?
It suffices to understand that internalization of secreted in vivo synthesized S protein into antigen-presenting cells (APCs) will provide cognate and noncognate T help to immunodominant epitopes on the free-circulating S protein and S protein expressed at the surface of the mRNA-transfected target cells, respectively. Abs to the latter have therefore much lower affinity and are the first to be recalled upon the administration of mRNA vaccine booster doses. As they will subsequently bind (with low affinity) to the immunodominant determinants on the free circulating S protein (i.e., once the latter is released from the mRNA-transfected cell), the subdominant antigenic determinants will be able to outcompete the immunodominant epitopes for assistance from memory T helper cells (recalled as a result of internalization of S protein into APCs) to recall their corresponding, broadly cross-functional memory Bcells. The neutralizing anti-S Abs (NAbs) recalled as a result of the original Wuhan-Hu spike memory(i.e., the ‘hidden’ original antigenic sin) imprinted by the mRNA vaccine have low affinity and are directed at conserved but less immunogenic S-associated domains. So, repeated boosting with mRNA-based vaccines will merely drive the immune system to repeat commitment of the ‘hidden’ antigenic sin. Consequently, mRNA booster injections will expedite immune escape by enabling immune refocusing to be repeated. As illustrated in the figure attached at the bottom, immune refocusing subsequently triggers the elicitation of low affinity infection-inhibiting Abs targeted at more conserved domains. So, regardless of the S version comprised in the mRNA vaccines, the mRNA booster vaccine doses facilitate humoral immune pressure on shared (i.e., variant-nonspecific) antigenic domains that contribute to viral neutralizability and infectiousness. Massive mRNA booster campaigns will therefore accelerate immune escape long before enhanced maturation of the recalled, poorly matured memory Bcells takes place in germinal centers (as equally described in several recent publications).
As mRNA boosters (as well as vaccine breakthrough infections) facilitate immune pressure on variant-nonspecific domains, the type of immune escape they indirectly promote is no longer determined by specific characteristics of the dominantly circulating SC-2 variant. This explains why we’re now witnessing more and more NAb-resistant, highly infectious variants co-circulating in the population.Lastly, as immune refocusing shifts the immune response to conserved domains with very different antigenic characteristics, it is not surprising that ‘mutation spotters’ consider the mutations to reflect ‘large scale’ immune escape.
End of master class...
Conclusion: Given the deep immunological incompetence of our leading scientific, public health and regulatory experts, one can easily predict that there will be many more plans for empiricism and injecting yet other experimental formulations than there are lucid brains. We should not forget, though, that mankind has never been in control of this pandemic and that this is even less the case as their rational experimentation continues. Indeed, the more man mismanages the pandemic by scientifically irrational immune interventions, the more (and the faster) the virus is evolving towards teaching a lesson in immunology that will hopefully be remembered by the future generation of scientists to come.History, however, will not be as mild as I am with the quotes of those who thought to learn from inconsiderate and dangerous experiments conducted on humans.
As someone who has also been watching this play out since day 1 (and watching guys like Geert, Knut Wittkowski, Robert Malone, etc. scream into the void since the beginning), I totally relate to your frustration.
Bossche was one of the few i knew instantly to be honest, ive read about viruses for two decades and knew the risks of variants with normal jabs let alone these monstrosities that would never stop transmission. these pfrauds are repulsive to anyone with integrity.
cheers for showing them up